Me with Master Parkinson's Cycling Coach Kathy Helmuth
This is without a doubt the most worthwhile project I've ever had the privilege to be involved in.
Over one million people in the USA suffer from the debilitating effects of Parkinson’s Disease. As of today, there is no known cure for Parkinson’s Disease, however, regular exercise has shown to help with the reduction of the symptoms associated with Parkinson’s Disease in many of those afflicted.
We feel Indoor Cycling is the safest and most effective form of exercise available.
The National Parkinson Foundation’s most recent study identified that 61 percent of people with Parkinson’s suffer from depression, with symptoms that ranged from mild to severe.
Exercise has been proven as an effective treatment for major depressive disorder (MDD), and now there is sufficient research to help doctors prescribe the proper dose of exercise for depressed patients… again, we feel Indoor Cycling is the best form of exercise.
But there are very few clubs or studios offering Indoor Cycling classes specifically for people with Parkinson’s Disease. And for good reason; there are only a handful of fitness professionals trained to properly conduct these classes — we plan to change that!
We're looking for committed fitness professionals to join our army of Parkinson’s Cycling Coaches, who will provide these hugely beneficial classes!
Earn 0.5 ACE CEC's
Meet Master Parkinson's Cycling Coach Kathy Helmuth and learn how you can train to become an ACE accredited Parkinson's Cycling Coach by listening to our announcement podcast below.
Interested in becoming a Parkinson's Cycling Coach?
Coaching a room full of Parkinson’s people is very different from teaching a traditional Indoor Cycling class… so different that we describe your future role as that of a coach, not an Instructor. Classes are coached off the bike, with you working the room, addressing individual needs and motivating your class.
To qualify for this training you'll need to possess a verifiable combination of the following prerequisites:
#1. Current Certification in CPR and AED
AND
#2 Current National Group Fitness Certification — ACE, AFAA, NETA or similar
OR
Current Personal Training Certification — ACSM, NASM, NETA or similar
OR
BS in Exercise Science or related Medical field
OR
Athletic / Endurance Coaching Certification — USA Cycling, ITCA, USAT or similar
2 or more years experience in conducting indoor cycling classes is helpful, but not mandatory for this program.
We feel these qualifications will provide a strong foundation to the training we provide, resulting in quality Parkinson’s Cycle Coaches.
This is an online training program that will take ~ 5 hours to complete. It's a combination of written articles, audio interviews and video demonstrations.
Join our army by clicking here to start your training as a Parkinson’s Cycling Coach.
Questions?
You can email Coach Kathy: kathy@parkinsonscyclingcoach.com or feel free to call her (941)-313-0004
Click here to learn more about the initial research that discovered how Indoor Cycling can help reduce the symptoms of Parkinson's Disease.
I'm not kidding. On the first day of Registered Dietitian School, I think every RD student must be taught to recommend the Registered Dietitian Breakfast: orange juice, yogurt and granola, often with berries.
I wish I could tell you this is a joke, but over many years, I've heard this recommendation from virtually every RD I've known or heard speak to groups. (And I've known a bunch. It's my business.) I'm suspicious when a group espouses exactly the same thing.
It has always driven me crazy, and still does. For one thing, they consider yogurt protein.
If you're thinking that yogurt IS protein, please understand they've been making this ridiculous recommendation for decades — long before the recent Greek yogurt trend started. That's important to keep in mind.
Before the craze, all yogurt – even the unflavored, unsweetened kind – was mostly carb with only a smidgen of protein. No yogurt had enough protein to compensate for the sugar in the OJ, the berries and the granola, especially when combined with the lactose in the yogurt. Yet RDs were blithely, shamelessly recommending it.
Even since the popularity of Greek yogurt, though, it's a bad recommendation because it's made with no specifications, no qualifiers. Sure, SOME Greek yogurts actually have enough protein to be considered protein food, but many do not. They're called Greek only because they've been created to feature that creamy texture that's considered characteristic of Greek-style yogurts. People really like them, but their protein content is relatively low.
And after all these years, non-Greek varieties of yogurt don't have much protein. They never did.
None of these food facts, however, has stopped RDs from recommending this infamous breakfast. Consistently, too, even though it's basically sugar, sugar, sugar and sugar. I even see it recommended in articles that offer breakfast suggestions for both regular folks and athletes. Some of the articles display pretty color photos of the breakfast.
In my humble opinion, the pretty picture doesn't make the sugar go away. It doesn't increase the protein content of the meal.
Again, the type of yogurt is almost never specified or clarified. But even telling the reader or the listener that it should be “Greek” won't fully help. Not when there are too many Greek-style yogurts available – and when, as previously mentioned, many of them have very little protein.
So which recommendation would make me stop ranting about, and railing against, the Registered Dietitian Breakfast? RDs could tell clients who want to try that meal to look for yogurt brands that contain between 18 and 22 grams of protein per serving. And lose the OJ.
How simple is that?
Okay, I freely admit RDs know some important stuff for sure, and many have their clients' welfare in mind at all times. Nevertheless, I'd give anything to meet even one who doesn't recommend this same breakfast. It absolutely has to be the first lesson they ever learn in RD school. How else could you explain such a bizarre phenomenon?
If it weren't part of the RD curriculum, why would they all say the same thing? Why would they have recommended it years before any yogurt, anywhere, had much protein?
You have to wonder, though: why would any curriculum include granola?
Avoiding unnecessary sugar and getting enough protein are only two keys to a healthy lifestyle. I help people conquer food addictions so they can keep moving forward (no matter what) with their goals to lose weight, improve their heath dramatically, transform their relationship with food, and stay that way. I'm available for coaching, lectures, workshops. Please visit http://www.foodaddictionsolutions.com.
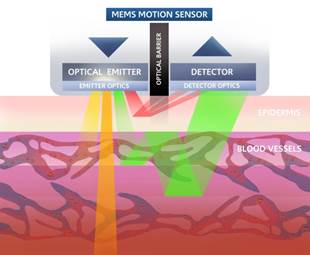
The Scosche armband heart rate strap uses optical sensors to “see” the pulses of blood flow in the blood vessels in your arm. Groundbreaking technology and pretty cool stuff if you ask me. Anything to get rid of those monitor chest straps will be an improvement. I feel this will result in a greater number of people training more effectively. You can read an earlier post where I describe the Scosche as possibly the best heart rate monitor strap option for participants in our classes that include any of the new Indoor Cycles with power consoles – except the Keiser M3 or M3i.
The new Apple iWatch uses the same optical sensor technology and it will be interesting to see how the two match up.
Jon Ham is a fitness consultant to Scosche and has written a detailed comparison between what he sees as the differences between the Scosche and the iWatch. You can read it here. [Understand that Jon's comments about the iWatch are based on information provided by Apple – the iWatch isn't available for purchase yet.]
As a side note, I've been trading emails with a former Schwinn Master Trainer who's involved in the iWatch project and (fingers crossed) I hope to interview him about the fitness applications of the iWatch once it's released.
The part I found most interesting in Jon's article was the part about data collection
Is the Apple Watch Designed to be a Continuous Heart Rate Monitor for intense exercise?
The way I saw it, In Tim Cook’s presentation, the Apple Watch was shown to be an excellent Activity/Life monitor, where movement, lifestyle, and general health were emphasized, and not heart rate training. I could be wrong, but I think Apple knows heart rate is not going to be super accurate during exercise with the Apple Watch, therefore they built the Watch around making a great interface for activity monitoring – IE: how often you stand up throughout the day, pedometer information, etc. This will surely play out to be a thorn in the side of FitBit and other activity monitors, but I don’t think it poses a threat to serious heart rate training athletes.
Data Centralization
I think Apple knows their job is to centralize the data collected from accurate sensors, not to necessarily create the sensor itself – except for activity monitoring. For example, Health Kit will allow all connected apps to push data that has been collected from different sensors directly into Apple’s Health App. I don’t see Apple getting into the Blood Pressure monitor or blood glucose monitor business any time soon, but apps that monitor blood pressure and blood glucose can push their data to Apple Health. I DO like the way the Apple Health App will centralize that information into one health app, along with other health related metrics. It makes sense to have all that data in one centralized location. The bottom line is that you should be able to use other heart rate sensors to do your workout and gather accurate data, you won’t be confined to only using the Apple Watch to collect accurate heart rate data.
Time will tell if Jon is accurate about this and if so, there's a chance we'll want to be wearing both an iWatch and a Scosche armband when we exercise.
You probably know how I came up with the title of this article. Several years ago, a popular book advocated chocolate consumption based on various factors, some of them unique to women. Hormone changes during PMS, menopause and stress were given as examples. Trust the body and give in to your cravings, the author told us! Indulging is better than depriving ourselves. Fat and carbs like bread and chocolate are the body’s natural feel-goods. (Yes, it really says that.)
Where are the anti-gluten, anti-processed food champions when we need them?
The good thing about the book was the extensive bibliography. I researched, read and cited a few of the references in my dissertation. Still, the author’s conclusions are flawed. For instance, she says cravings reflect the body’s needs. It’s a common theory, but it’s just not the case with processed, addictive foods.
So I hope you haven’t been recommending chocolate for your students, even if it’s PMS time!
Why talk about this not-so-new book? Because cocoa is news. No doubt you’ve read about, heard about, and talked about the benefits of cocoa, particularly dark, unsweetened, 70% cacao. They’re everywhere lately: the antioxidant benefits due to the specific flavonoids in cocoa, called polyphenols.
A quick summary of the benefits includes decreases in all of these: blood pressure, insulin resistance, excess clotting, diabetes risk factors, and the risk of cancer, stroke, and coronary heart disease.
In addition, cocoa promotes increased HDL (good) cholesterol and improvements in vascular health and gut bacteria, which thrive on the polyphenols. Cocoa can prevent oxidation of LDL, which contributes to arterial disease when unchecked. It even seems to inhibit fluid secretion in the small intestine, so research may soon show it to be effective in treating diarrhea.
Other health benefits are reduced fatigue and improved mood, both due to cocoa’s natural theobromine (similar to caffeine). Another mood-elevating chemical in cocoa is phenylethylamine, sometimes likened to the feeling of being in love.
What I won’t do — send me your hate mail now — is what the book’s author did, namely recommend chocolate. Even 70% dark chocolate.
Why not? The drawbacks of sugar are too great. In fact, sugar can singlehandedly reverse almost every one of the benefits of cocoa listed above.
But there’s not much sugar in 70% chocolate, you say.
I specialize in sugar addiction, so I look at sugar’s consequences differently. Recently, at someone else’s seminar, a participant offered her opinion that “sugar is bad in large quantities.” You’ll never hear me argue with that! Yet sugar can be bad even in small quantities because of its sneaky effects.
One sneaky effect of sugar is to increase appetite. Another sneaky effect is to change food preferences. Both of these are due to endorphins, which are often overlooked when people talk about health or food.
And what then? Your students may eat an “innocent” amount of chocolate and find themselves wanting more food in general AND more endorphin-triggering foods — such as sugar of all types.
This is how the quantity of sugar can go way up when students eat chocolate for its “health” benefits. Health becomes the excuse for eating sugar. And that’s why I won’t recommend it (no matter who does).
But I will — and do — strongly recommend cocoa. Dark, unsweetened, 70% cacao will let you reap the benefits of cocoa without the drawbacks of sugar. Please tell your students.
It’s squash season! Winter squash — almost all of them — are among my favorite foods. They’re an excellent source of starchy carbs, which are necessary for training, and don’t add the undesirable elements of sugar or gluten.
People ask how I cook squash, and my answer is shocking but true. I microwave. (As mentioned in previous posts, I’m a lazy cook but determined to eat healthful foods.) One safety note: larger squash, such as butternut, can be difficult to cut when raw. Most roasting/baking instructions require cutting the squash in half before placing it in the oven, so be careful. If you decide to be lazy like me, you can microwave without cutting first.
Acorn squash seems to be everywhere these days. It can be eaten as part of a quick pre-training meal. The meal could include any protein source you choose, from dinner leftovers to vegetable protein powder. Reheat the acorn squash, if desired, and top it with some raw, organic coconut oil. It’s a fast, healthy meal and can get you through a tough workout.
Stuffed acorn squash makes a nice dinner side dish. You can, of course, use virtually anything you like to stuff it. One combination I’ve played with is brown rice, wild rice, chopped vegetables, and pine nuts. If you go easy on seasonings, this could also serve as part of the pre-training meal above.
Another terrific squash is delicata. It can be substituted for acorn squash in either dish above and offers a little variety.
And how about spaghetti squash? It can be eaten just like any other squash, seasoned whichever way you prefer. But it also has that added fun-factor because it can be used exactly like spaghetti and topped with your favorite sauce to make a gluten-free “pasta.”
My favorite squash dish combines two winter standards. Butternut has a fantastic flavor but is often watery. Kabocha (aka Japanese pumpkin) has a drier, firmer texture but tastes bitter. Combining the two is easy. Cook both, let them cool, and discard the seeds. Scoop out the squash from each one, place it in a bowl, and use a potato masher to blend them. It’s really quick. Pour out the water from the butternut squash as necessary.
The taste of this combo is good enough to be eaten plain with no seasoning. But, obviously, you can season it if you want, with any seasonings you choose.
Whether you already like squash or try it for the first time it this season, you might miss it (as I sometimes do) the rest of the year. Here’s one way around that. A few years ago, I discovered canned, organic pumpkin. Look for a brand that contains pumpkin and absolutely nothing else. You can treat it exactly the way you would oatmeal or quinoa in my no sugar, no-bonk breakfast suggestion from a previous post. Season it according to your preference. I tend to use cinnamon at breakfast, but sea salt, freshly ground pepper, allspice, nutmeg, curry, and many other seasonings can work quite well anytime. If you stock up on several cans, you’ll have it year-round.
My plan this year is to try some of the squash varieties I’ve never tried before. If you have a favorite recipe, please feel free to pass it along to us. And please let me know how squash works as part of your pre-workout meal.
Have you ever noticed that some of your students react more strongly to sugar than others? That they seem to want it more often, crave it frequently, and want more even after they’ve eaten some? The reasons are genetic. I love that because it takes all the “blame” off the person and de-personalizes the reaction by making it chemical. We can’t be blamed for something we can’t control, right?
As an indoor cycling instructor, you may hear all about students’ problems with sugar. You’re also in a unique position to help them. Your students know you, trust you, and follow your recommendations.
So what is this genetic, chemical thing that goes on in people who are susceptible to sugar addiction? It’s in two parts — carbohydrate sensitivity and sugar sensitivity.
Carb sensitivity simply means exaggerated insulin secretion to sugar and some other carbs. The extra insulin can cause glucose to drop, causing cravings. The cravings are typically for foods that will raise glucose quickly. Sugar is an obvious culprit in that regard. The glucose drop can also trigger hunger, so it’s likely that the carb-sensitive person will crave sugar, eat it, and eat quite a bit of it.
Who’s likely to be carb sensitive? Typically people with a family history of one or more of these: alcoholism, diabetes (including mature-onset), hypoglycemia, hypertension, or obesity. Another factor is central adiposity (apple-shaped body). That apple shape is the typical characteristic of men, but women with that body type are more likely to be carb-sensitive.
The other aspect — sugar sensitivity — is about neurochemistry. People who are sugar-sensitive seem to have low baseline levels of several brain chemicals — beta-endorphin (or endorphins), dopamine, and serotonin. To simplify (oversimplify!), the fact that those 3 chemicals are lower than normal makes these people feel crummier than normal.
Who is likely to be sugar-sensitive? People with a family history of alcoholism, other addictions, depression or other mood disorders, or a personal history of PTSD (post-traumatic stress disorder).
Let’s return to sugar. When we eat sugar, we get a brain release of beta-endorphin. That triggers a dopamine response because the two tend to go together. But when a sugar-sensitive person eats sugar, the beta-endorphin response is greater than normal — and so is the dopamine release.
Their serotonin will be exaggerated, too — because of carb sensitivity and the high insulin release. The more insulin we secrete, the more tryptophan (the amino acid used to make serotonin) travels to the brain, and the more serotonin we produce. It’s pretty linear. So carb-sensitives — who release extra insulin when they eat sugar — end up making a lot more serotonin.
And what does all of this have to do with addiction?
Dopamine and beta-endorphin are involved in the good-feeling, reward part of addiction (including sugar addiction). That means people who are sugar-sensitive may feel rotten without sugar, but hugely better than normal when they eat it. Obviously, that’s pretty reinforcing. It encourages repeat behavior, both in animals and in humans.
Then there’s serotonin. Serotonin is involved in seeking behavior — how much trouble we’re willing to go through to get the addictive substance we want. Once again, the exaggerated response comes in here. Extra insulin leads to extra serotonin, and that leads to stronger seeking.
To recap, it kinda works like this for a carb-sensitive, sugar-sensitive person: She/he may feel crummy without sugar. The giant-sized reward caused by extra-high dopamine and beta-endorphin makes Ben & Jerry’s seem pretty appealing in the middle of the night. Reinforcement from eating it may provoke that desire on many nights, while the extra serotonin is what makes someone drive to the store in a bathrobe at 2:00 am to get it.
What I love about this hormonal and neurochemical viewpoint is that it takes all judgment off the person, who can’t fight those genetics any more than we can fight our eye color. There’s nothing wrong with feeling compassion, rather than judgment, for someone’s compulsions. Judgment never helps anyone, although compassion certainly can.
What besides compassion can help your students? Changes in nutrition are most important, but if you’re not comfortable tackling addiction, you can still help. Don’t underestimate the organized, structured workouts you offer in your classes.
You may already know that workouts increase brain levels of beta-endorphin, dopamine and serotonin. (More on serotonin and training in a future post.) Encourage consistent participation from your sugar-addicted students, especially any who are in recovery from alcohol or other substances.
Even if they don’t want to work out some days, your class will help them that day AND in the long run — and make you feel great that what you do so well can be so beneficial for them.